
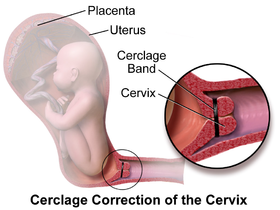
The treatment consists of a strong suture being inserted into and around the cervix early in the pregnancy, usually between weeks 12 to 14, and then removed towards the end of the pregnancy when the greatest risk of miscarriage has passed.
In women with a prior spontaneous preterm birth and who are pregnant with one baby, and have shortening of the cervical length less than 25 mm, a cerclage prevents a preterm birth and reduces death and illness in the baby. There is no evidence that cerclage is effective in a multiple gestation pregnancy for preventing preterm births and reducing perinatal deaths or neonatal morbidity.
Types
There are three types of cerclage- A McDonald cerclage, described in 1947 is the most common, and is essentially a pursestring stitch used to cinch the cervix shut; the cervix stitching involves a band of suture at the upper part of the cervix while the lower part has already started to efface. This cerclage is usually placed between 16 weeks and 18 weeks of pregnancy. The stitch is generally removed around the 37th week of gestation.[5] This procedure was developed by the Canadian Gynecologist and Obstetrical Pathologist and Surgeon, Ellice McDonald (1876–1955)
- A Shirodkar cerclage is very similar, but the sutures pass through the walls of the cervix so they're not exposed. This type of cerclage is less common and technically more difficult than a McDonald, and is thought (though not proven) to reduce the risk of infection. The Shirodkar procedure sometimes involves a permanent stitch around the cervix which will not be removed and therefore a Caesarean section will be necessary to deliver the baby. The Shirodkar technique was first described by V. N. Shirodkar in Bombay in 1955. In 1963, Shirodkar traveled to NYC to perform the procedure at the New York Hospital of Special Surgery; the procedure was successful, and the baby lived to adulthood.
- An abdominal cerclage, the least common type, is permanent and involves placing a band at the very top and outside of the cervix, inside the abdomen. This is usually only done if the cervix is too short to attempt a standard cerclage, or if a vaginal cerclage has failed or is not possible. However, a few doctors (namely Arthur Haney at the University of Chicago and George Davis at the University of Medicine and Dentistry of New Jersey) are pushing for the transabdominal cerclage to replace vaginal cerclages, due to perceived better outcomes and more pregnancies carried to term. A c-section is required for women giving birth with a TAC. A transabdominal cerclage can also be placed pre-pregnancy if a patient has been diagnosed with an incompetent cervix
- After the cerclage has been placed, the patient will be observed for
at least several hours (sometimes overnight) to ensure that she does not
go into premature labor. The patient will then be allowed to return
home, but will be instructed to remain in bed or avoid physical activity
(to include coitus) for two to three days, or up to two weeks.
Follow-up appointments will usually take place so that her doctor can
monitor the cervix and stitch and watch for signs of premature labor.
Risks
While cerclage is generally a safe procedure, there are a number of potential complications that may arise during or after surgery. These include:
- risks associated with regional or general anesthesia
- premature labor
- premature rupture of membranes
- infection of the cervix
- infection of the amniotic sac (chorioamnionitis)
- cervical rupture (may occur if the stitch is not removed before onset of labor)
- injury to the cervix or bladder
- bleeding
- Cervical Dystocia with failure to dilate requiring Cesarean Section
- displacement of the cervix
Results
The success rate for cervical cerclage is approximately 80-90% for elective cerclages, and 40-60% for emergency cerclages. A cerclage is considered successful if labor and delivery is delayed to at least 37 weeks (full term).For women who are pregnant with one baby (a singleton pregnancy) and at risk for a preterm birth, when cerclage is compared with no treatment, despite there being a reduction in preterm birth, there is no reduction in deaths of the baby before or after birth, or reduction in illness in the baby after birth. There is no evidence that cerclage is effective in a multiple gestation pregnancy for preventing preterm births and reducing perinatal deaths or neonatal morbidity.

No comments:
Post a Comment